| dc.contributor.advisor | Bakken, Linda Nilsen | |
| dc.contributor.author | Holte, Andreas Søberg | |
| dc.date.accessioned | 2021-11-04T17:42:09Z | |
| dc.date.available | 2021-11-04T17:42:09Z | |
| dc.date.issued | 2021 | |
| dc.identifier | no.usn:wiseflow:2398807:38837650 | |
| dc.identifier.uri | https://hdl.handle.net/11250/2828014 | |
| dc.description.abstract | Bakgrunn: Med en aldrende befolkning og større press på helse- og omsorgstjenesten er det behov for en endring. Et av målene til samhandlingsreformen var å gi mer helhetlige pasientforløp og øke brukerens deltagelse i prosessen. En måte å gjøre dette er ved personorientert helsearbeid, hvor man aktivt inndrar pasienten i forløpet, benytter seg av samvalg, brukerens egne mål. Dette kan gjøres lettere ved å bruke subjektive kartleggingsverktøy, som potensielt kan gi en mer rød tråd i tjenestene.
Formål: Formålet med studien var å prøve ut og vurdere subjektive kartleggingsverktøy som allerede var implementert på et rehabiliteringssenter. Tidligere studier har påpekt behovet for å prøve ut disse på en bredere demografi med eldre brukere, til tross for at de allerede er implementert i stor skala. Problemformulering: Hvordan kan subjektive kartleggingsverktøy komplementere objektive utfallsmål ved rehabilitering av sårbare eldre brukere? For å finne ut av dette vil studien fokusere på følgende forskningsspørsmål: I hvilken grad samsvarer de objektive og subjektive testene? Hvor godt er de subjektive testene egnet for ulike pasientkarakteristika? Er det demografiske forskjeller på den subjektive scoringen?
Hvilke egenopplevde aktiviteter er brukerne mest opptatt av å forbedre?
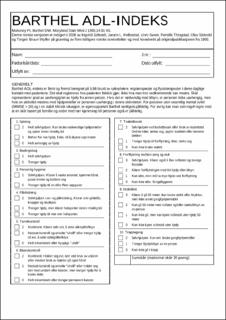
Metode: Kohortestudie med retrospektiv og prospektiv design. Studien undersøkte brukere på en kommunal rehabilitering og all data ble innhentet i 2020. Det ble brukt fire kartleggingsverktøy, to subjektive og to objektive. De subjektive var Patient-specific functional scale og EQ5D5L. De objektive var Berg balansetest og Barthel ADL index. Dataene ble innhentet av fysio- og ergoterapeuter som jobbet på de ulike avdelingene. Totalt var det 68 brukere i utvalget etter eksklusjon. Eksklusjonskriterier: språk (norsk og stor grad av afasi), kognisjon og samtykke. Resultater: Det ble funnet varierende grad av samvariasjon mellom de subjektive og objektive testene, fra ingen til høy samvariasjon. Høyest var samvariasjonen mellom Bergs og PSFS (r=0.55**), Barthel og EQ2 (r=0.41**) og mellom Barthel og PSFS (r=0.35**) Det var større samvariasjon i kartleggingsverktøyene som testet de samme fysiske dimensjonene. Ingen store forskjeller på gruppenivå; hva gjelder samvariasjon eller scoring på testene. Med unntak av delspørsmålet EQ3 hvor menn subjektivt opplevde en signifikant gjennomsnittlig høyere bedring enn kvinnene. PSFS-aktivitetene som var viktigst for brukerne ble kategorisert i ICFs-rammeverk og prioriterte i kronologisk rekkefølge: aktivitetsnivå (38.8%), funksjonsnivå (38.1%) og deltagelsesnivå (23.1%).
Konklusjon: Subjektive og objektive kartleggingsverktøy har stor variasjon av samvariasjon. Det ser ut til at de vurderer forskjellige aspekter av brukernes funksjonsevne, noe som igjen får frem flere dimensjoner i rehabiliteringsprosessen. Dette fremhever viktigheten av å supplere med subjektive kartleggingsverktøy hos eldre og sårbare brukere.
Subjektive kartleggingsverktøy gjør det lettere for brukeren å aktivt delta i rehabiliteringsprosessen, noe som fremmer bruken av personorientert helsearbeid.
Studien har vist at sårbare eldre er mer opptatt av flere dimensjoner enn aktivitetsnivå ut ifra ICF-kategoriseringen. Til tross for at denne vektes høyest anser de i høyere grad viktigheten av funksjonsnivå og deltagelsesnivå enn andre studier har funnet hos brukere med vesentlig høyere fysisk funksjon enn i dette utvalget.
Nøkkelord: Subjektive kartleggingsverktøy, objektive kartleggingsverktøy, personorientering, samvariasjon, PSFS, EQ5D5L, Berg balansetest, Barthel ADL index. | |
| dc.description.abstract | Background: With an aging population and greater pressure on the health- and care service, a change is needed. One of the goals of the «collaboration reform» was to provide more holistic patient processes and increase patient participation in the process. One way to do this is through person centered care, where you actively involve the patient in the process, use co-selection, the patient's own goals. This can be made easier by patient-reported outcomes measures (PROS), which can potentially provide a more common thread in the services.
Objectives: The purpose of the study was to test and evaluate PROS that had already been implemented at a rehabilitation center. Previous studies have pointed to the need to try these out on a broader demographic with older patients. Problem statement: How can PROS complement performance-based outcome(PBOM) measures in the rehabilitation of frail elderly users? To find out, the study will focus on the following research questions: To what extent do the PROS and PBOM correlate? How well are the PROS suitable for different patient characteristics? Are there demographic differences in scoring of the PROS? Which self-perceived activities are the users most concerned with improving?
Method: Cohort study with retrospective and prospective design. The study examined users in a municipal rehabilitation and all data were collected in 2020. Four outcome-measures were used, two PROS and two PBOM. The subjective were Patient-specific functional scale and EQ5D5L. The objectives were the Berg balance test and the Barthel ADL index. The data were collected by physiotherapists and occupational therapists who worked in the various departments. In total, there were 68 users in the sample after exclusion. Exclusion criteria: language (Not beeing able to talk/understand Norwegian and a large degree of aphasia), cognition and consent.
Results: A varying degree of correlation was found between PROS and PBOM, from none to high correlation. The highest correlation was between Bergs and PSFS (r = 0.55 **), Barthel and EQ2 (r = 0.41 **) and between Barthel and PSFS (r = 0.35 **). There was greater correlation in the tools that tested the same dimensions. No major differences at group level; in terms of correlation or scoring on the tests. With the exception of the sub-question EQ3 where men subjectively experienced a significantly higher average improvement than women. The PSFS activities that were most important to users were categorized into ICFs frameworks and prioritized in chronological order: activity level (38.8%), function level (38.1%) and participation level (23.1%).
Conclusion: PROS and PBOM have a great variety of correlation. It seems that they assess different aspects of the users' ability to function, which in turn brings out several dimensions in the rehabilitation process. This emphasizes the importance of supplementing with PROS for elderly and frail patients.
PROS makes it easier for patients to actively participate in the rehabilitation process, and promote the use of person-centered care.
The study has shown that frail elderly people are more concerned with more dimensions than activity level based on the ICF categorization. Despite the fact that they consider this as most the important dimension, they consider the importance of functional level and participation level to a greater extent than other studies have found in users with significantly higher physical function than in this sample.
Keywords: Patient-reported outcome measures, performance-based outcome measures, person-centered care, correlation, PSFS, EQ5D5L, Berg balance test, Barthel ADL index. | |
| dc.language | nob | |
| dc.publisher | University of South-Eastern Norway | |
| dc.title | Bruk av subjektive kartleggingsverktøy på sårbare eldre brukere innlagt på rehabilitering. | |
| dc.type | Master thesis | |